Hormones
Progesterone and Progestogens
Benefits, side effects and how to choose the right progestogen.

Body-identical micronised progesterone is the modern first-line choice for most women on HRT. This guide explains its benefits, side effects, and when synthetic progestogens or a Mirena coil may be preferred.
Progesterone and its synthetic cousins (progestogens or 'progestins') sit at the heart of women's hormonal health — regulating the menstrual cycle, supporting pregnancy, protecting the womb lining during HRT and influencing mood, sleep and bone health. The differences between natural body-identical progesterone and the many synthetic progestins are subtle but clinically important, and matching the right form, dose and route to the woman in front of you is often what separates a successful HRT regimen from one she abandons.
Natural progesterone vs synthetic progestogens
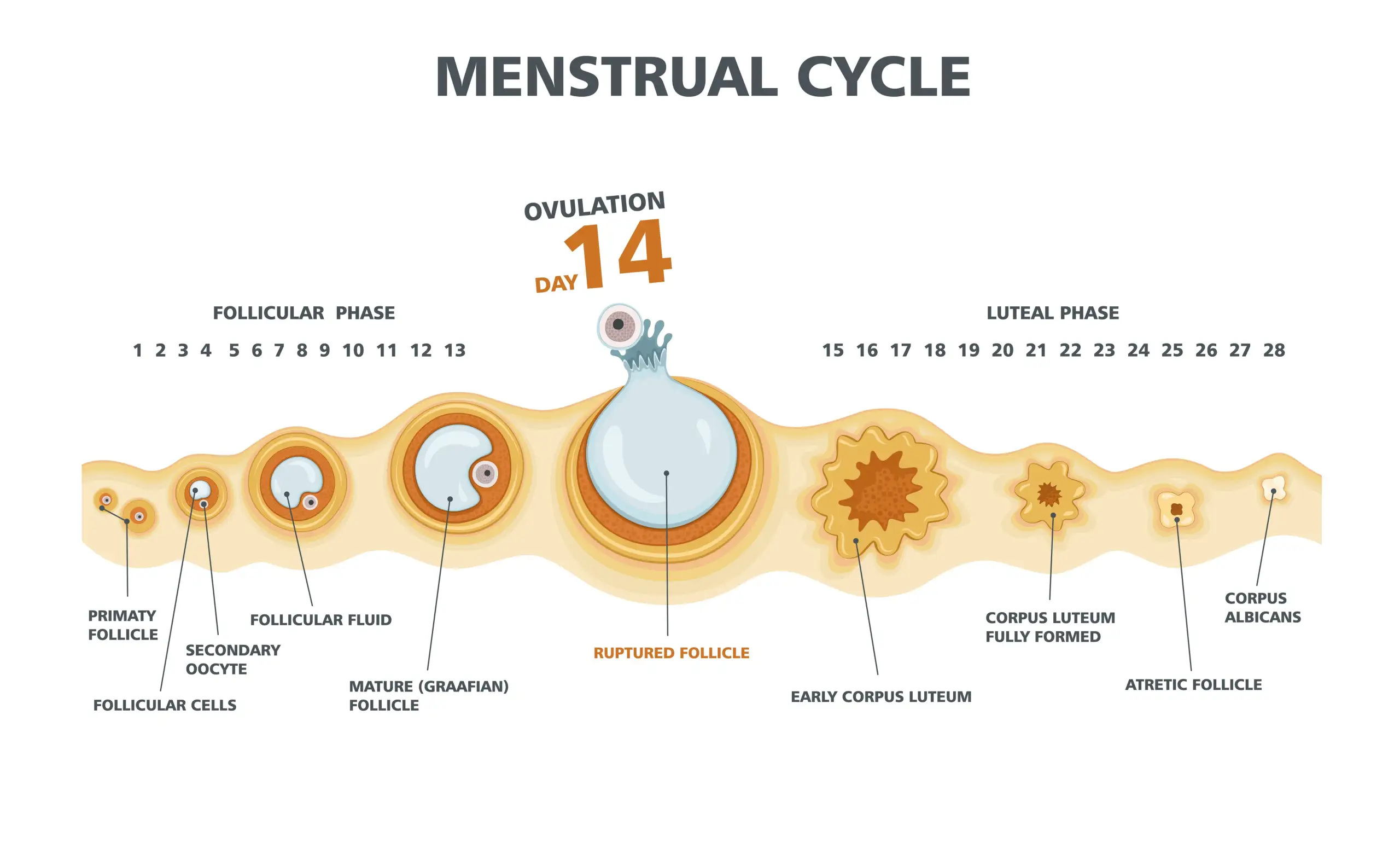
- Natural progesterone is a steroid hormone made by the ovaries (specifically the corpus luteum after ovulation) and, in pregnancy, by the placenta.
- It acts on progesterone receptors found throughout the reproductive tract, brain, bone and vascular tissue — which is why its effects reach well beyond the uterus.
- Synthetic progestogens ('progestins') were developed from the 1940s onwards because natural progesterone is very poorly absorbed by mouth without special processing.
- Progestins are structurally modified to improve oral absorption and potency, but the modifications can also introduce androgenic, anti-androgenic or mineralocorticoid effects — which drives their different side-effect profiles.
The main forms used in the UK
- Micronised (body-identical) progesterone — Utrogestan and Gepretix; oral capsules or off-licence vaginal use. Chemically identical to the body's own hormone.
- First-generation progestins — norethisterone, medroxyprogesterone acetate (MPA). Potent, sometimes androgenic (acne, hirsutism in a small number of women).
- Second-generation — levonorgestrel and norgestrel. Backbone of the Mirena, Levosert and Kyleena intrauterine systems and many combined pills.
- Third-generation — desogestrel, gestodene, norgestimate. Lower androgenicity; some studies suggest a slightly higher VTE risk than levonorgestrel.
- Fourth-generation — drospirenone. Anti-androgenic and mildly diuretic; useful in PCOS and women prone to fluid retention.
- Others — dienogest (particularly effective for endometriosis) and nomegestrol acetate.
Why body-identical micronised progesterone is often preferred in HRT
- Bioidentical structure — metabolised by the body in the same way as its own progesterone, giving a more physiological response.
- Cardiovascular profile — does not appear to blunt the beneficial effect of oestrogen on lipids and has a neutral/favourable effect on blood pressure.
- Breast cancer signal — the French E3N cohort found no clear increase in breast cancer risk in the first 5 years of combined HRT using micronised progesterone or dydrogesterone, unlike older synthetic progestins.
- Sleep — oral micronised progesterone is metabolised to allopregnanolone, a GABA-active neurosteroid, which is why most women take it at bedtime and often notice better sleep.
- Tolerability — many women who felt low, bloated or flat on older synthetic progestogens do far better on Utrogestan or a Mirena.

Why progesterone is essential alongside oestrogen
- Oestrogen alone thickens the womb lining and, over time, raises the risk of endometrial hyperplasia and cancer.
- Progesterone or a progestogen counteracts this and keeps the lining thin — this is 'endometrial protection'.
- Women who have had a hysterectomy don't need progesterone for the womb, but some still take it for sleep, mood or perceived breast benefits.
- Typical HRT dosing: oral Utrogestan 100mg nightly continuously (post-menopause) or 200mg for 12 nights each month (cyclical, in perimenopause).
Common side effects — and what we can do about them
- Drowsiness — usually desirable; taken at bedtime.
- Breast tenderness and bloating — often settles by 8–12 weeks; if not, we look at dose, route or a switch to Mirena.
- Mood changes ('progesterone intolerance') — irritability, tearfulness or low mood in a minority of women, more common in those with a history of PMDD, PND or previous reaction to the pill.
- Headaches or vivid dreams — usually mild and short-lived.
- Irregular bleeding in the first 3 months of a continuous regimen — expected; needs review if it persists beyond 6 months.
Progesterone intolerance — why some women are more sensitive
- Genetic variation in hormone-metabolising enzymes (e.g. CYP3A4, CYP2C19) changes how quickly progestogens are cleared.
- Neurotransmitter sensitivity — progestogens act on GABA and serotonin systems; women with PMDD, PND or anxiety may feel this more.
- Oestrogen-to-progesterone ratio matters as much as absolute dose.
- Prior exposure (pill, previous HRT) and body composition also modulate response.
Options when standard oral Utrogestan isn't tolerated
- Vaginal Utrogestan (off-licence, but widely used in BMS-specialist practice) — bypasses the liver and often much better tolerated for mood and bloating while still protecting the womb lining.
- Mirena intrauterine system — five years of contraception AND the progestogen half of HRT in one device; ideal in perimenopause, heavy bleeding, or clear progesterone intolerance.
- A change of preparation — sometimes dydrogesterone (Femoston) or a low-dose combined patch (Evorel Sequi) suits better.
- Adjusting the regimen — cyclical vs continuous, or a lower oestrogen dose alongside.
Beyond HRT — where progestogens are also used
- Contraception — levonorgestrel, desogestrel, drospirenone (pills, coils, implants, injections).
- Heavy menstrual bleeding — norethisterone short-term, or a Mirena as a long-term first-line option.
- Endometriosis — dienogest (Visanne) is particularly effective; continuous progestogens suppress the cycle and reduce pain.
- Menstrual regulation and cycle control in perimenopause.
Key takeaway
Progesterone is not just an add-on for endometrial safety — it is a hormone in its own right, and choosing the right type, route and dose is often what makes HRT feel good rather than just tolerable. In clinic we start with body-identical Utrogestan or a Mirena for most women, and switch route or type quickly if it doesn't suit — no one should give up on HRT because of a progestogen that isn't right for them.
How Dr Awal approaches this in clinic
Every consultation starts with your full story — symptoms, cycle, medical history, family history and what you've already tried. From there we look at whether hormonal treatment, non-hormonal options, lifestyle changes or a combination will give you the best result, and we tailor the plan to your age, risk factors and preferences.
- A detailed 60 minute first appointment — no rushed 10-minute slots.
- Evidence-based recommendations aligned with NICE NG23 and BMS guidance.
- Body-identical HRT considered first-line where appropriate.
- Shared-care letters sent to your NHS GP so treatment can continue affordably.
- Follow-up at 3 months to fine-tune your regimen and address side effects.
- Ongoing annual reviews so your plan evolves with you.
Common questions we hear about this
Do I need to be at a certain age to be seen?
No. We see women in early perimenopause (often late 30s and 40s), through post-menopause and beyond. Age alone doesn't decide whether treatment is right — symptoms, health history and goals do.
Will my GP continue the prescription?
In most cases yes. After your consultation we send a detailed shared-care letter with the diagnosis, treatment plan and rationale so your NHS GP can prescribe on the NHS. Not every practice accepts shared care — we'll discuss this in your appointment.
What if I've tried HRT before and it didn't suit me?
Very common — often the type, dose or route wasn't right rather than HRT itself. We review what you've tried, why it didn't work, and adjust accordingly. Many women who thought HRT wasn't for them do well on a different preparation.
How long will I need to stay on treatment?
There is no set upper time limit for HRT. Current BMS and NICE guidance supports continuing HRT for as long as the benefits outweigh the risks for you personally. We review this together every year so you stay in control of the decision.
Where do you see patients?
All consultations at Pause and Co Healthcare are conducted securely via video, allowing us to support patients anywhere in the UK. Prescriptions and shared care arrangements are managed in the same way, regardless of your location.
About the author
Dr Nadira Awal is a British Menopause Society Advanced Menopause Specialist with 15+ years' NHS and private experience. She holds the BMS Advanced Certificate in Menopause Care, sits on the BMS Programme Planning Group, and advises the UK Government Menopause Strategy Group. Read her full profile.
Sources & further reading
General information only — not a substitute for personalised medical advice. Always speak to your GP or a menopause specialist about your own situation.
Talk it through
Book a private consultation with Dr Awal
Get evidence-based, personalised advice on progesterone and progestogens and any related concerns.
Related in Hormones
Continue reading

Importance of Female Sex Hormones
Oestrogen, progesterone and testosterone across the life course.
Read guide

Testosterone and Menopause
The role of testosterone in women's health and how to access treatment.
Read guide

Non-Hormonal Options
Evidence-based alternatives when HRT isn't right or preferred.
Read guide